

ACA Subsidies in Limbo: What the Senate Framework Means for Patients
Congress races to salvage affordable coverage as millions face premium spikes and negotiators clash over cost-sharing provisions

The enhanced Affordable Care Act (ACA) premium tax credits expired on January 1, 2026, and millions of Americans are now facing the consequences. According to the Kaiser Family Foundation, subsidized enrollees are seeing their out-of-pocket premium payments increase by an average of 114%. For a single mother in social work like Katelin Provost, that means watching her monthly premium jump from $85 to nearly $750, a ninefold increase that forces an impossible choice between her own coverage and her daughter's.
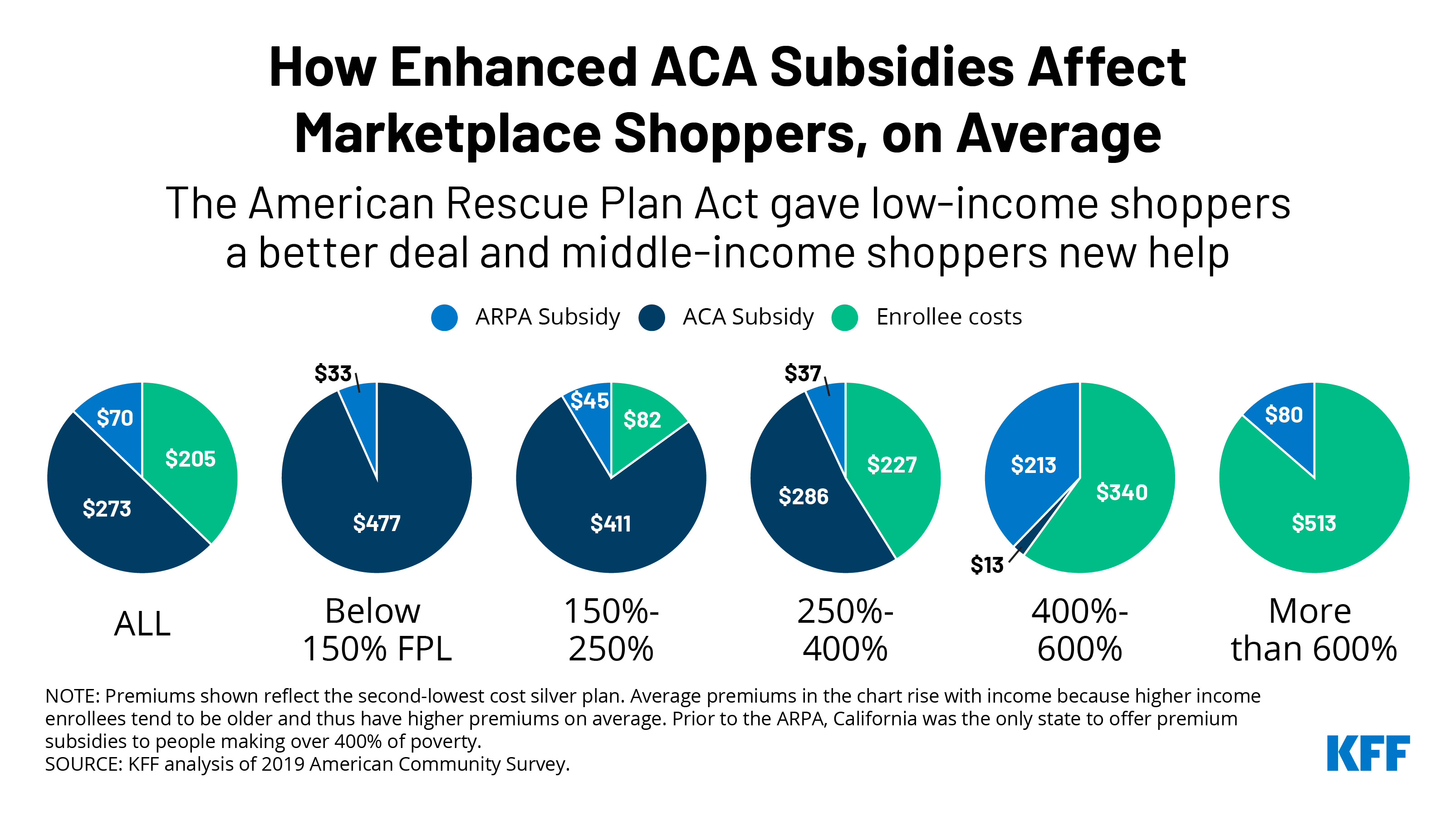
This is the reality for more than 20 million Americans who benefited from the enhanced subsidies first enacted in 2021 as a COVID-19 pandemic response. The Wall Street Journal reports that roughly four in ten ACA enrollees had been paying nothing toward their premiums under the enhanced credits—more than double the share in 2020. That era ended last week, and Congress is now scrambling to respond amid growing political pressure and the specter of another government shutdown deadline on January 30.
The House Vote: Forcing the Issue
Last Thursday, the House passed a three-year extension of the enhanced subsidies, a bill that has no chance of becoming law in its current form. The Senate rejected an identical measure in December. So why hold the vote?
The answer lies in a procedural rebellion that caught House leadership off guard. Four swing-district Republicans—Reps. Mike Lawler of New York and Robert Bresnahan, Brian Fitzpatrick, and Ryan Mackenzie of Pennsylvania—signed a Democratic discharge petition to force the vote over Speaker Mike Johnson's objections. Last Wednesday, nine Republicans joined Democrats on a procedural motion to advance the bill.
These centrist Republicans are calculating political survival. As Rep. Fitzpatrick told The Hill, "Everyone's lamenting discharge petitions. There's an easy way to fix that: Put bills on the floor that have majority support. It's not hard." The vote serves a strategic purpose: it creates a legislative vehicle the Senate can amend and sends a clear signal that inaction carries electoral consequences in November's midterms.
The Senate Framework Takes Shape
While the House engages in political theater, a bipartisan Senate group led by Sens. Bernie Moreno (R-Ohio) and Susan Collins (R-Maine) has been negotiating a compromise. According to Politico, legislative text could be ready as early as today.
The emerging framework includes a two-year extension of enhanced subsidies with several Republican-demanded reforms. The Wall Street Journal outlines the key elements: an income cap excluding households earning more than 700% of the federal poverty level (approximately $225,000 for a family of four), a requirement that enrollees pay at least $5 per month toward their coverage, and $100,000 fines on insurers who sign up "phantom enrollees" without their knowledge. In the second year, enrollees would have the option to direct their subsidy funds into a pre-funded health savings account instead of having them flow to insurance companies.
The framework also reportedly includes measures to directly fund cost-sharing reductions (CSRs), which could generate significant savings. The Committee for a Responsible Federal Budget estimates that direct CSR funding would reduce deficits by over $50 billion over a decade while lowering silver plan premiums by 10% to 20%. This would end the practice of "silver loading," where insurers inflate silver plan premiums to compensate for CSR costs the federal government stopped paying in 2017.
Sen. Moreno told NPR, "We're in the red zone. But that does not mean a touchdown. It could mean a 95-yard fumble."
The Barriers to a Deal
Two sticking points threaten to derail negotiations: abortion coverage and the elimination of $0 premium plans.
On abortion, Republicans want explicit language preventing subsidies from flowing to plans that cover the procedure. Democrats counter that current law already addresses this concern—ACA plans that cover abortion must charge enrollees a separate $1 per month, segregating federal funds from abortion services. Sen. Ron Wyden (D-Ore.) warned Fox News, "I am not going to open the door to Hyde, given what happens and what has been seen historically when you do that. If you open the door, it will get drafty in a hurry."
President Trump complicated matters when he told House Republicans to be "flexible on Hyde," drawing pushback from conservatives. Sen. Moreno has since indicated the framework does not change current abortion policy, calling the issue "peripheral" to the core negotiations.
The second obstacle carries more direct implications for patient access. The proposed $5 monthly minimum premium—designed as an anti-fraud measure—would eliminate $0 premium plans that currently cover millions of low-income enrollees. Sen. Wyden called this a "rate hike" affecting 8 million people. Sen. Jeanne Shaheen (D-N.H.) noted, "Data shows that you lose a lot of people at the lowest income levels when you do that."
This concern is grounded in evidence. The NIH Clinical Guidelines on Antiretroviral Therapy are direct: "Out-of-pocket costs for people with HIV can be prohibitive, creating a barrier to the initiation and continuation of ART. Cost sharing results in higher rates of people not initiating ART, prescription abandonment at the pharmacy, decreased adherence, and more frequent drug discontinuation." The guidelines note that in 2022, the CDC's Medication Monitoring Project found that among people with HIV who had stopped taking antiretroviral therapy, 34% reported that money or insurance problems contributed to stopping treatment. For people managing chronic conditions requiring consistent care, even modest cost-sharing can disrupt treatment continuity with serious downstream consequences for both personal health and public health goals.
Why This Matters for People Living with Chronic Conditions
The evidence on cost-sharing and health outcomes should inform how we evaluate any compromise. The Commonwealth Fund's 2023 Health Care Affordability Survey found that 37% of marketplace enrollees reported delaying or skipping needed care due to cost in the prior 12 months. Among those who delayed care, 61% said a health problem got worse as a result. One-third of marketplace enrollees reported paying off medical debt.
These affordability challenges fall disproportionately on certain communities. The Center on Budget and Policy Priorities notes that 23% of Black enrollees and 18% of Hispanic enrollees in private insurance reported problems paying medical bills, compared to 15% of white enrollees.
For people living with HIV, coverage continuity directly affects health outcomes. The NIH Clinical Guidelines emphasize that "health insurance and prescription drug coverage can directly affect clinical outcomes for people with HIV; changes to coverage can result in lapses in viral suppression and should be anticipated as best possible." The guidelines specifically warn that disengagement from care occurs more frequently during transitions in coverage, including when people switch insurance plans or experience changes in employment status. With wholesale acquisition costs for commonly prescribed single-tablet antiretroviral regimens ranging from approximately $2,800 to $4,700 per month, the stakes of coverage disruption are substantial.
As CANN's December analysis detailed, New York City's 2024 HIV surveillance data showed diagnoses rising for the fourth consecutive year, with 86% of new diagnoses among Black or Latino people and 48% of those interviewed lacking health insurance. The Ryan White HIV/AIDS Program and AIDS Drug Assistance Programs (ADAPs) provide critical safety net support, but these programs work best when complementing stable insurance coverage rather than substituting for it.
The KFF analysis of proposed Medicaid cost-sharing requirements offers a window into what happens when cost barriers are introduced for vulnerable populations. Under a maximum cost-sharing scenario, Medicaid expansion enrollees with three or more chronic conditions could face average annual costs of $1,248—potentially exceeding the 5% of income cap for those at 100% of the federal poverty level.
What Comes Next
Any Senate deal requires 60 votes to overcome a filibuster, meaning at least seven Democrats must join all 53 Republicans, or significant bipartisan support must materialize. Sen. Moreno has indicated he needs 35 Republican senators on board to feel confident in the level of GOP support. Senate Majority Leader John Thune has said any deal must get a "big vote" among Republicans.
The political calendar adds pressure. The January 30 government funding deadline looms, and neither party has appetite for another shutdown after last fall's 43-day standoff. An extended open enrollment period would likely accompany any deal, giving people who dropped coverage due to premium spikes a chance to re-enroll.
For advocates, the coming days demand close attention. The specific legislative text—particularly provisions around minimum premiums, income verification, and any changes to covered services—will determine whether a compromise actually improves access or introduces new barriers. Contact your Senators to emphasize that affordability must remain central to any reform. Monitor for the final text expected early next week. And prepare to help community members navigate an extended enrollment period if one materializes.
The enhanced subsidies enabled record ACA enrollment of 25.2 million in early 2025, according to KFF data. What happens in Congress over the next two weeks will determine whether that progress holds or unravels, and whether the people who depend on affordable coverage can continue accessing the care they need.
This article was written for Community Access National Network (CANN) and originally published at hiv-hcv-watch.com.